 Home
Home Back
Back| Classification | Clinical Manifestation |
|---|---|
| Type A | 1. Unilateral or bilateral common iliac artery stenosis 2. Unilateral or bilateral short segment stenosis of the external iliac artery ≤3cm 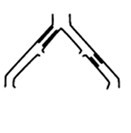 |
| Type B | 1. Short segment stenosis of the infrarenal aorta ≤3cm 2. Unilateral common iliac artery occlusion 3. Unilateral or multiple stenoses of the external iliac artery not involving the common femoral artery (total length 3-10cm) 4. Unilateral external iliac artery occlusion not involving the internal iliac artery and the origin of the common femoral artery 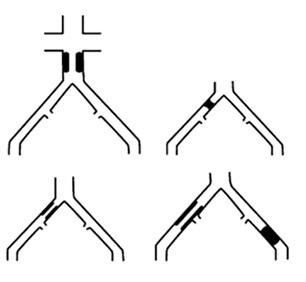 |
| Type C | 1. Bilateral common iliac artery occlusion 2. Bilateral external iliac artery stenosis not involving the common femoral artery (total length 3-10cm) 3. Stenosis of the unilateral external iliac artery involving the common femoral artery 4. Unilateral external iliac artery occlusion involving the internal iliac artery and/or the origin of the common femoral artery 5. Unilateral external iliac artery occlusion with severe calcification, involving or not involving the origin of the internal iliac artery and/or the common femoral artery 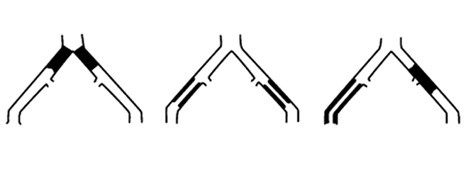 |
| Type D | 1. Infrarenal aorta-iliac artery occlusion 2. Extensive lesions in the abdominal aorta and bilateral iliac arteries requiring treatment 3. Multiple extensive stenoses involving the unilateral common iliac artery, external iliac artery, and femoral artery 4. Occlusion involving the unilateral common iliac artery and external iliac artery 5. Bilateral external iliac artery occlusion 6. Iliac artery stenosis combined with abdominal aortic aneurysm requiring treatment but unsuitable for endovascular therapy, or other lesions requiring open surgery for the abdominal aorta or iliac arteries 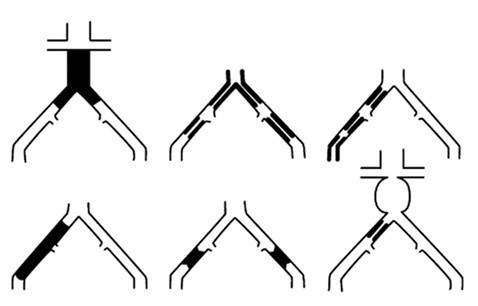
|
Explanation
"Type A" lesions are localized with good expected outcomes, and should be treated using endovascular techniques;
"Type B" lesions are slightly extended, but balancing the risks and expected patency of surgery versus endovascular treatment, the latter remains the primary choice;
"Type C" lesions have good outcomes through surgical reconstruction, but for patients with high-risk factors, minimally invasive endovascular techniques can be considered;
"Type D" lesions should opt for surgical treatment.
